from : Laws of Fryette 다이어그램 | Quizlet
 |
 “Principles of Osteopathic Technic”American Academy of Osteopathy, 1980. First Edition 1954 ISBN (ASIN) B0006Y0VBI, (ASIN) B0007F1Y80 Hardcover. 246 pages. Perspective: Osteopathy, Osteopathic Principles, Spinal Mechanics |
| 구분 | 타입 1 (정상적 척추 움직임) |
타입 2 (비정상적 척추 움직임) |
| 척추후관절의 위치 | - Neutral position 즉, •Neutrality(중립) basically means where the facet joints are idling
-Fryette, 1918년- |
Non neutral position |
| 척추뼈가 굽힘 혹은 폄이 되어 있는가? | 없음 | 있음 |
| 짝운동 (가쪽굽힘 + 돌림) 방향은 같은가 반대인가? | 반대 방향 | 동일 방향 |
| 척추뼈 몸통의 돌림 방향은 볼록한 쪽인가 오목한 쪽인가? | 오목한 방향으로 회전함 | 볼록한 방향으로 회전함 |
| 임상에서의 모습 | 가쪽으로 만곡됨 (측방 만곡0 |
- 굽힘시: 특정 분절의 가시돌기가 돌출됨 - 폄시: 특정 분절의 가시돌기가 함몰됨 |

1st Law - ERS / FRS
side bending and rotation happen to the same side: primary dysfunction
N = neutral or easy flexion (articular facets are in neutral position; parallel and not touching)
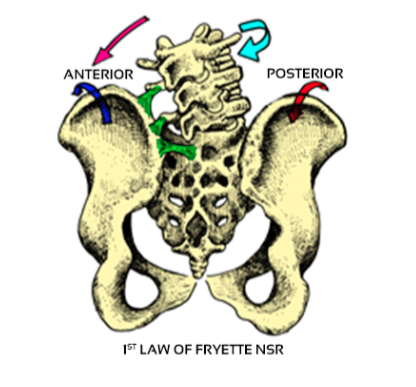
>>When vertebrae are in neutral/easy flexion , side bending and rotation occur to opposite sides
2nd law - NSR
sidebending and rotation happen to opposite sides: secondary adaptive dysfunction

■ Laws of Fryette
1st law: NSR, ESR or FSR
N = neutral or easy flexion
(articular facets are in neutral position; parallel and not touching)
>>When vertebrae are in neutral/easy flexion side bending and rotation occur to opposite sides
2nd law: ERS or FRS
>>When vertebrae are in hyper flexion (F) or hyper extension (E) side bending and rotation occur to the same side.
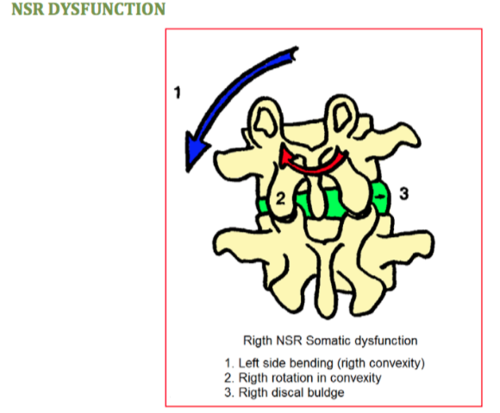
■ Biomechanics - NSR right
■ Biomechanics -ERS / FRS left

■ NSR
-group dysfunction: 2-3 segments involved or more rotate in the same direction
-multifidi muscles span 1-3 vertebrae and cause rotation to the same side (causative for NSR dysfunction)
- Adaptive dysfunction (not primary) usually over or under a primary dysfunction
-type of dysfunction seen in scoliosis
-will correct after the primary lesion has been treated.
-If doesn't correct means its chronic and has become a compensation and requires treatment.
-psoas major responsible for group NSR L1-5
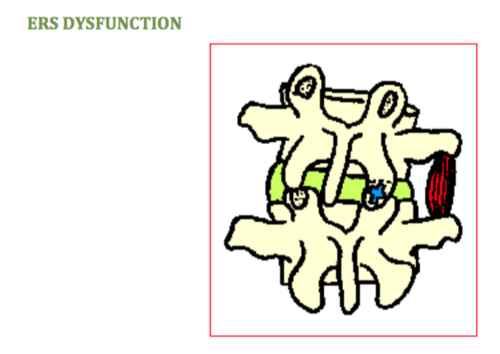
■ ERS
- Vertebrae is fixated in a hyperextended position so forward flexion is painful or difficult
- ipsilat multifidi is responsible for the fixation on the dysfunction side
- facet is imbricated (closed) goal of manipulation is to open
- TVP is posterior and low on the side of imbrication
-find ERS in childs pose position as vertebrae does not accept flexion but disappears and will hide in extension
-active side bending look for "break" in arc of spine; if break occurs to only one side - means there is fixation on the opposite side facet
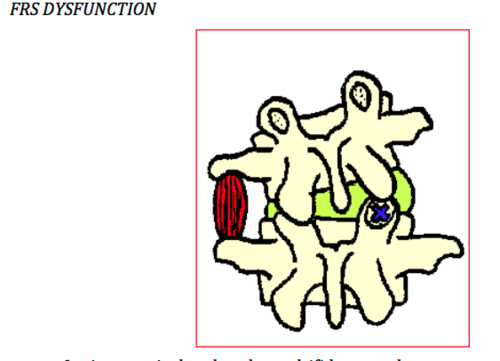
■ FRS
-Vertebrae is fixated in hyper flexion; facet cannot close it is stuck open (disimbrication)
-pain can be intense and gait is antalgic with an inability to straighten or extend spine
-vertebrae does not accept extension movements
-found in sphinx position and disappears in childs pose
- mechanical problem (disimbrication) occurs on the opposite side of rotation - disc is moved posterolaterally and blocks the opening of the facet on opposite side of rotation.
-spasm of multifidus muscle on side of rotation fixes the vertebrae in this position
-greatest parameter is usually extension or side bending (often referred to as laterality)
-goal of manipulation is to close the disimbrication
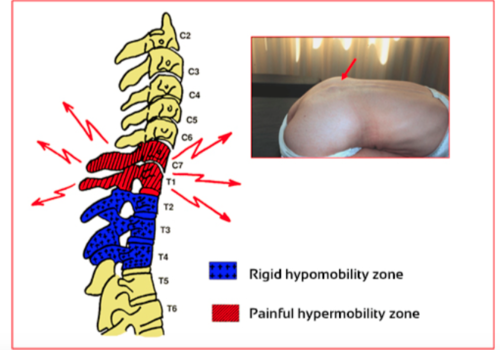
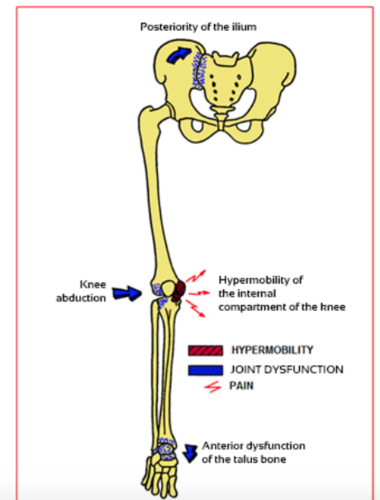
■ Compensating hype / hypermobility
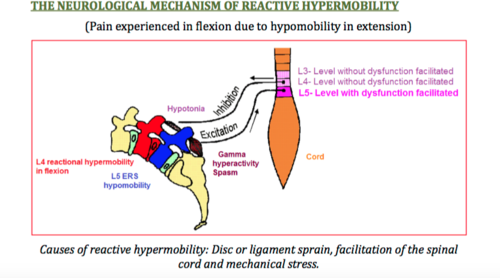
■ Characteristics of reactive hyper mobility
-common to find vertebral lesions in thoracic spine that are asymptomatic early stages
- highly pathogenic b/c affects on dura mater, cranial sacral movement, vasomotricity (visceral impact) and symptomatic over functioning in areas above or below
-EX: stiffness T1-5 causes hyper mobility in C7 or C6 and results in cervical brachial neuralgia
-hypermobile areas prone to degenerative arthritis
■ Hyper mobility
■ What is an adaptation? causes?
■ What' s difference between adaptation and compensation?
it always following a primary lesion. It will always take place in a neutral position and in a group (NSR)
ALL adaptation neutral dysfunctions affect a group
Causes:
-somatic dysfunction
-short leg
-reflex (antalgic posture)
-adaptations reduce body ability to adapt to other things; lowers defence
-reversible dynamic lesion (doesn't always need treatment)
- primary lesions are asymptomatic while multiple adaptations generate symptoms
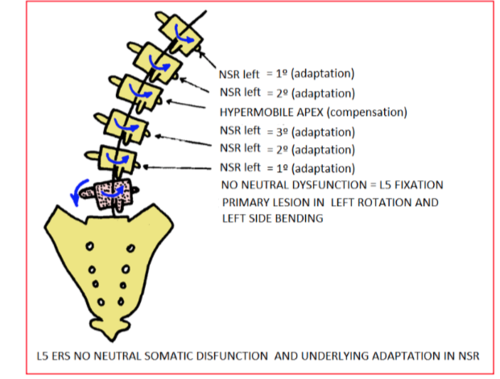
■ What is Martindales Law?
Applies to adaptive groups of vertebrae in a non-neutral lesion (primary vertebrae in a non-neutral lesion allows for correction of the adaptive group)
FRS - primary vertebrae is the upper vertebrae of adaptive group; perform a lateral mobilization of the primary vertebrae to correct adaptive group
ERS - primary vertebrae is bottom of group; de-rotate starter vertebrae to correct adaptive group
NSR - rest of the group (not primary) are NSR dysfunctions. Rotation of the entire group is produced in the convexity.
if adaptation does not correct after the primary vertebrae has been treated then de-rotate apex of the curve vertebrae to invert/reduce convexity.
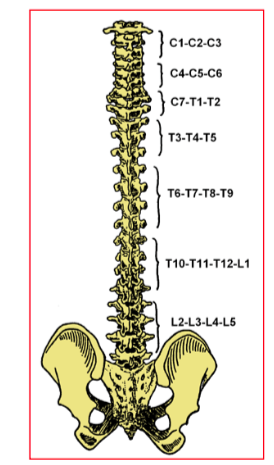
groups: C1-3, C4-6, C7-T2, T3-5, T6-9, T10-L1, L2-5
'3_물리치료 Healing is Voltage' 카테고리의 다른 글
| EMI, Electro-Acuscope 80 ... 피드백 제어 미세 전류 시스템 (1) | 2023.01.10 |
|---|---|
| 🫦허리 통증 ; 허리가 너무 아파요 ~❤️💕 허리뼈-기능장애 LUMBAR SPINE : 비중위 기능장애 Non-Neutral Dysfunction (Example: L4 ERS left) (0) | 2022.11.04 |
| 🔰🔰 Spinal motion : Spinal engine - Serge Gracovesky (세르지 그라코베스키) (0) | 2022.10.02 |
| 🔰🔰 Spinal motion : Spinal motion (0) | 2022.09.30 |
| 🔰🔰 Spinal motion : 오른쪽 허리, 오른쪽 엉덩이가 아픈 경우 ; 아픈 이유 ? (0) | 2022.09.30 |


